Objective 1-Factors that Influence Older Adults Lives
In the last three decades the older adult population (those 65 years of age and older) has grown twice as fast as the rest of the population according to Lewis, Dirksen, Heitkemper, Bucher and Camera (2011). Medicare is a federally funded health insurance program for people ages 65 years and older( Lewis et al., 2011). Nicholas and Hall (2011) state at the time of this writing there are 43 million eligible older adults and total enrollment is predicted to exceed 70 million lives by the year 2050. Per Nicholas et al., (2011), at Medicare’s inception, the priority health care needs of older adults were addressed by providing insurance coverage for catastrophic illness, hospital based treatment and access to fee-for-service physician services. It has not been until recently that screening and prevention have been incorporated in to the mission of Medicare (Nicholas et al., 2011). Per Lewis et al., (2011), in March 2010 the United States passed the health care reform bill and under Medicare, deductibles and co-payments for preventive services would be eliminated; preventive services would be free.
According to Lewis et al., (2011), daily living with chronic illness is a reality for many older adults and most persons 65 years of age and older have at least one chronic condition and many have multiple conditions. According to Nicholas et al., (2011), rising federal and personal health care expenditure have refocused prevention efforts in the hopes that early detection and treatment of health conditions will minimize more costly attempts at advance disease treatment. Nicholas et al., (2011) also state increased longevity has led to an imperative to provide preventive services for health issues that specifically emerge in later life. According to Nicholas et al., (2011), adherence to national guidelines for screening and prevention for older adults is particularly poor for geriatric syndromes (such as urinary incontinence screening and falls risk assessment), as compared to traditional disease-specific screening (e.g. hypertension).
According to Nicholas et al., (2011), we are now better positioned to improve the preventive care for older adults than at any previous time in history. “Three phenomena are converging to create this opportunity for health care providers. 1) It is estimated that by 2012, about 10,000 Baby Boomers will turn 65 each year. This cohort will be better informed about health, more pro-active about their own prerogatives, and highly likely to embrace prevention as a keystone of their future medical care. These individuals will be among the first generations to recognize that longevity per se is a Pyrrhic victory if those addition years gained are characterized by frailty, disability and declining quality of life. 2) The implementation of Patient Protection and Affordable Care Act, US health care providers are now able to offer older adults a robust range of preventive services not previously provided because of inadequate preventive service reimbursement. 3) The years 2010-2011 mark the publication of new age-specific guidelines for the utilization of screening and preventive services for older adults. In addition to disease-specific guidelines to promote longevity, a Geriatrics Task Force of the United States Preventive Services Task Force is developing specific new guidelines to emphasize evidence-based evaluation of geriatric conditions that affect quality of life, the first of which is an approach to falls prevention” Nicholas et al., (2011).p. 499

Environmental safety is crucial in the health maintenance of the older person according to Lewis et al., (2011). "The older adult is prone to accidents because of normal sensory changes, slowed reaction time, decreased thermal and pain sensitivity, changes in gait and balance, and medication effects" Lewis et al., (2011). p.75 Falls, motor vehicle accidents, and fires are the common causes of accidental death in older adults. Another environmental problem arises from the older person's impaired thermoregulation system that cannot adapt to extremes in environmental temperatures; the body of an older adult can neither conserve nor dissipate heat as efficiently as younger adults and therefore both hypothermia and hyperthermia occur more readily (Lewis et al., 2011). This age group accounts for the majority of deaths during severe cold spells and heat waves according to Lewis et al., (2011). According to Nicholas et al., (2011) new guidelines addressing primary care interventions to prevent falling in all older adults is now available and it is assumed that for any given geriatrics condition it may be necessary to both screen for multiple risk factors, and implement multiple interventions to significantly improve outcomes such as reduced falls and improved functional status.
Lewis et al., (2011) states the use of assistive devices should be considered as an intervention for the older adult. Many older adults use or could benefit from the use of assistive devices such as dentures, glasses, hearing aids, walkers, wheelchairs, adult briefs or protectors, adaptive utensils, elevated toilet seats, and skin protective devices. These tools and devices should be included in the patient’s care plan and the nurse is in a position to ensure the correct and consistent use of these devices, Lewis et al., (2011). According to Lewis et al., (2011), computerized assistive devices can be used to help patients with speech difficulties following strokes, and small electronic devices can serve as memory aids; monitoring can also locate a person with dementia who has wandered away from home or long term care facility.
According to Lewis et al., (2011), persons over age 65 are less likely to live in metropolitan areas than younger person and face special challenges. According to Lewis et al., (2011), "five barriers to health care access are transportation, limited supply of health care workers and facilities, lack of quality health care, social isolation and financial limitations". p. 67. In areas where homelessness is increasing, the number of older adults who are homeless is increasing as well. Key factors that are associated with homelessness include (1)having a low income, (2) reduced cognitive capacity, (3) living alone, and (4) lack of affordable housing this according to Lewis et al., (2011). Per Lewis et al., (2011), many older adults stay in their place of residence and do not move to a different home or geographic location when ability to do self-care declines. Lewis et al., (2011) also state that many older adults are on fixed incomes, they may need housing assistance through property tax relief, assistance with home repair, and fuel payment. Community resources that are abundant and accessible support the ability of older adults to maintain their privacy while finding companionship and maintain a sense of belonging (Lewis et al. 2011) p. 70-71. According to Lewis et al., (2011), when it is no longer safe, affordable or practical for an older adult to remain in his or her home, other housing arrangements are available, depending on physical and cognitive ability. Per Lewis et al., (2011), older adults with special care needs include people who are homeless, in need of assistance with ADLs, cognitively impaired, homebound, and /or no longer able to live at home. The older adult may be served by adult day care, home health care and long term care (Lewis et al. 2011). According to Wasserman (2010), imagine a community where people of all ages and cultures live together; where health status is evaluated on a continuum; where there are programs designed to elevate the best of each person thereby enabling their contributions, as they are able; where older people are considered valuable asset to the community offering themselves as mentors to teens and teens to toddlers. Per Wasserman (2010), thriving communities that bring together diverse resources seem to be a clear alternative to the state institutional approach that has marked our history.
Per Lewis et al., (2011), aging is defined as the progressive loss of function. "Biological aging can be viewed as a balance of positive factors such as healthy diet, regular exercise, and coping resources and negative factors such as obesity, unhealthy lifestyle (smoking), chronic illness, and stress that exceeds the individuals's coping resources" (Lewis et al., 2011). According to Black (2011), despite the recognition that people are living longer that ever before and requiring more interventions and support at the end of life, there is still a limited number of studies that have high-lighted the preferences, priorities, or wishes of patients approaching this point of their lives. Further investigation into this area is necessary for trying to meet, or at least to understand, the wishes and preference of dying people. This would be to the benefit of not only patients, but also their families, caregivers and the wider professional organization who may care for and support them. According to Lewis et al., (2011), end of life is the period of time during which an individual copes with declining health from a terminal illness or from the frailties associated with advance age even if death is not clearly imminent.
According to Pijnenburg and Leget (2007), life is an intrinsic good, and individuals who are ready to accept all ethical objections are not different from those who choose to live in luxury without feeling the moral obligation of justice. Also, the question must be discussed to what extent life extension contributes to the public good. The concept of “public good” however is slightly ambiguous, Pijnenburg et al., (2007). The concept of common good entails a society where individuals inextricably bind up their own good with the good of the whole. It forces reflection on the question of whether living longer is good for me as a human being, and whether a society whose members have a much longer life than in the case at present would be a better society, Pijnenburg et al., (2007). Pijnenburg et al., (2007) state there is a moral challenge to expand our view of the common good to encompass good for all, worldwide. This expansion inevitable raises the urgent question of whether we can morally afford, as a question of moral integrity, to invest time and money in trying to extend our lives while sidelining the whole issue of unequal death, Pijnenburg et al., (2007). According to Lewis et al., 2011, research is directed at increasing both the average life span and the quality of life of older adults, it is hoped that new anti-aging therapies will be developed to slow down or reverse age-related changes that result in chronic illness and disability.
References:
Lewis, S., Dirksen, S., Heitkemper, M., Bucher, L. and Camera, I. (2011). Medical-
Surgical Nursing. Assessment and Management of Clinical Problems. St. Louis,
Missouri: Elsevier Mosby.
Nicholas, J. and Hall, W. (2011). Screening and preventive services for older adults. Mt.
Sinai Journal Medicine, 78(4), 498-508.
Black, J. (2011). What are patients’ priorities when facing the end of life? A critical
review. International Journal of Palliative Nursing, 17(6), 294-300.
Pijnenburg, M. and Leget, C. (2007). Who wants to live forever? Three arguments
against extending the human lifespan. Journal Medical Ethics, 33, 585-587.
Objective 2-Normal Age Related Changes in Older Adults
Who is old? According to Lewis et al., (2011), the answer to this question often depends on the age and attitude of the respondent. Age is a date in time and is influenced by many factors, including emotional and physical health, developmental stage, socioeconomic status, cultural and ethnicity, Lewis et al., (2011). Older adults with poor health report a higher perceived age and lower sense of well-being as compared with healthy older adults, Lewis et al., (2011). Myths and stereotypes about aging, found throughout society, are supported by media reports of problematic older adults. According to Lewis et al., (2011), myths and stereotypes regarding aging provide the basis of commonly held misconceptions that may lead to errors in assessments and unnecessary limitations to interventions. Ageism is a negative attitude based on age and leads to discrimination and disparities in the care given to older adults (Lewis et al. 2011). It is important to gain knowledge about normal aging and have increased contact with healthy independent older adults to avoid negative attitudes.
Lewis et al., (2011), state age related changes affect every body system. Changes are normal and occur as people age; however, the age at which specific changes become evident differs from person to person and within the same person, e.g. a person may have gray hair at age 45 but relatively unwrinkled skin at age 80, Lewis et al., (2011). The incidence of chronic illness triples after age 45 and most persons 65 years of age and older have at least one chronic condition and many have multiple conditions. The most common chronic conditions present in the older adult are hypertension, arthritis, heart disease, cancer and diabetes. Other common chronic conditions include vision loss, deafness and hearing impairment, Alzheimer's disease, osteoporosis, hip fractures, urinary incontinence, stroke, Parkinson's disease and depression (Lewis et al. 2011).
The frail elderly are older adults who, because of declining physical health and resources, are most vulnerable. Lewis et al., (2011), states the frail older adult has difficulty coping with declining functional abilities and decreasing daily energy. The frail older adult is especially at risk for malnutrition and problems with hydration status, both are related to factors such as living alone, depression and low income. Per Lewis et al., (2011), other factors such as declining cognitive status, inadequate dental care, sensory decreases, physical fatigue and limited mobility also add to the risks of malnutrition and dehydration.
Declining physical health is an important factor that influences cognitive impairment. The older adult who experiences sensory loss, heart failure or cerebrovascular disease may show a decline in cognitive functioning (Lewis et al. 2011). According to Lewis et al., (2011), an appropriate cognitive assessment includes functional ability, memory recall, orientation, use of judgement and appropriate emotional state. According to Vance, Graham, Fazeli, Heaton, and Moneyham, (2012), there are several definitions of successful aging, and all include some aspect of cognitive functioning. Physical health and comorbid conditions also affect cognitive health; unfortunately, concerns about physical health often eclipse cognitive health until one’s cognitive functioning begins to decline (Vance et al. 2012). Psychomotor functioning refers to reaction time (e.g., such as reacting to stimuli in a driving simulator), fine motor movements (e.g., sewing and buttoning a shirt), and gross motor movements (e.g., raising one’s hand and lifting one’s foot). Studies demonstrate that these abilities decline with age (Vance et al. 2012). According to Vance et al., (2012), some degree of age-related cognitive decline is a part of normal aging, this does not mean that it is necessarily inevitable for everyone to experience cognitive deficits that impair everyday functioning. Fortunately, evidence now demonstrates that interventions and strategies such as cognitive remediation therapy and lifestyle choices can actually improve and maintain cognitive health in older adults (Vance et al. 2012).
According to Nicholas et al., (2011), historically malnutrition, weight loss and frailty were the chief considerations in terms of weight management in older adults. Now overweight states and obesity are emerging as potentially far more serious health risk factors. The prevalence of obesity and its attendant morbidities is increasing in old persons as in younger cohorts. Approximately 20% of adults age 65 and older are obese, and the prevalence is likely to increase. Obesity is being increasingly recognized as a significant determinant in the accelerated onset and progression of cognitive disorders. A connection between obesity and muscle loss has been documented, obesity is associated with urinary incontinence in women, and significant psychosocial morbidity including isolation, loneliness and depression (Nicholas et al., 2011).
References:
Lewis, S., Dirksen, S., Heitkemper, M., Bucher, L. and Camera, I. (2011). Medical-
Surgical Nursing. Assessment and Management of Clinical Problems. St. Louis,
Missouri: Elsevier Mosby.
Vance, D., Graham, M., Fazeli, P., Heaton, K., and Moneyham, L. (2012). An overview
of nonpathological geroneuropsychology: implications for nursing practice and
research. Journal of Neuroscience Nursing. 44, 43-54.
Nicholas, J. and Hall, W. (2011). Screening and preventive services for older adults. Mt.
Sinai Journal Medicine, 78(4), 498-508.
Objective 3-Asthma
Asthma is a chronic inflammatory disorder of the airways which leads to recurrent episodes of wheezing, breathlessness, chest tightness, and cough, particularly at night or in the early morning. The clinical course of asthma is unpredictable, ranging from periods of adequate control to exacerbations with poor control of symptoms. According to Lewis et al., (2011), "the primary pathophysiologic process in asthma is persistent but variable inflammation of the airways. The airflow is limited because the inflammation results in bronchoconstriction, airway hyper responsiveness (hyper reactivity) and edema of the airways. Exposure to allergens or irritants initiates the inflammatory cascade. A variety of inflammatory cells are involved including mast cells, macrophages, eosinophils, neutrophils, T and B lymphocytes, and epithelial cells of the airways".
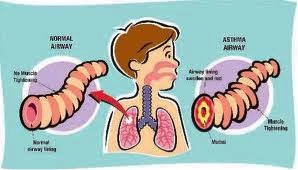
According to Lewis et al., (2011), as the inflammatory process begins, mast cells degranulate and release multiple inflammatory mediators, these effect the blood vessels, causing vasodilation and increasing capillary permeability. The resulting inflammatory process results in vascular congestion; edema formation; production of thick, tenacious mucus; bronchial muscle spasm; thickening of airway walls, and increased bronchial hyper responsiveness - this process is referred to as the early-phase response and can occur within 30-60 minutes after exposure to the allergen or irritant (Lewis et al., 2011). Late -phase response occurs 4 to 10 hours after the initial attack and can be more severe than the early-phase response and can persist for 24 hours or more. It is characterized by a self-sustaining cycle of inflammation. Airflow may be limited from the swelling of the airways with or without bronchoconstriction. Corticosteroids are effective in treating this inflammation (Lewis et al., 2011).
According to Lewis et al., (2011), asthma is characterized by an unpredictable and variable course from seemingly minor interferences in breathing to life-threatening episodes that can occur in the same person. An attack of asthma may have an abrupt onset, attacks may last for a few minutes to several hours. Between attacks the patient may be asymptomatic with normal or near-normal pulmonary function, depending on the severity of disease. According to Lewis et al., (2011), the clinical manifestations of asthma are wheezing, cough, dyspnea, and chest tightness after exposure to a precipitating factor or trigger. A result of bronchospasm, edema, and mucus in the bronchioles, the airways become narrower than usual and it takes longer for the air to move out of the bronchioles. This produces the characteristic wheezing, air trapping and hyperinflation (Lewis et al., 2011).
Per Lewis et al., (2011), the health care provider should consider the diagnosis of asthma if various indicators are positive, i.e., clinical manifestations, health history and peak flow variability or spirometry. Pulmonary function tests can be used to determine the reversibility of bronchoconstriction and thus establish the diagnosis of asthma. According to Lewis et al., (2011), the goal of asthma treatment is to achieve and maintain control of the disease. Once a patient is diagnosed, guidelines from the National Asthma Education and Prevention Program give direction on classification of severity and which medications the patient requires. Per Lewis et al., (2011), the current guidelines focus on (1) assessing the severity of the disease at diagnosis and initial treatment and then (2) monitoring periodically to achieve control of the disease. According to Lewis et al. 2011, patients in all classifications of asthma will require a short-term (rescue or reliever) medication - the short acting B2-adrenergic agonists(e.g., albuteral), are the gold standard and most effective. Patients with persistent asthma must be on a long-term or controller medication and inhaled corticosteroids(e.g., fluticasone) are the most effective class of drugs to combat the inflammation (Lewis et al., 2011).
According to Yan, Mu, Huang, Lou, and Wu (2012), asthma has a high prevalence among children and because of the characteristics of the disease; asthma may cause a variety of problems, such as school absenteeism or limited participation in activities. According to Liu, Gilsenan, Stanford, Lincourt, Ziemiecki, and Ortega (2010), asthma is a prevalent chronic medical condition and is the most frequent cause of hospitalization in children. in US school age children, in 2003, uncontrolled asthma led to an estimated annual loss of 12.8 million school days, or approximately 3.2 missed days of school for each student with asthma (Liu et al., 2010). According to Liu et al., (2010), all children with asthma should be screened for asthma control at every primary care visit, because many who come in for a non-respiratory related visit may be uncontrolled and can benefit from an asthma evaluation.
Nursing goals:
The child and family will receive appropriate support and education regarding the disease and it's management. Asthma education and awareness are important aspects of asthma management.
The child will engage in normal activities for age. According to Yan et al., (2012), studies have indicated that if children with a chronic disease are socially well adapted, they will perform better at school and have relatively high self-esteem; furthermore, they will also be better at managing their behavior.
References:
Lewis, S., Dirksen, S., Heitkemper, M., Bucher, L. and Camera, I. (2011). Medical-
Surgical Nursing. Assessment and Management of Clinical Problems. St. Louis,
Missouri: Elsevier Mosby.
Yang, B.H., Mu, P.F., Huang, C.M., Lou, H.L. and Wu, K.G. (2012). Relationship among asthma
knowledge, behavior management and social adaptation in school age children with asthma
in Taiwan. Nursing and Heath Sciences, 14, 165-172.
Liu, A., Gilsenan, A., Stanford, R., Lincourt, W., Ziemiecki, R., and Ortega, H. 2010. Status of asthma
control in pediatric primary care: results from the pediatric asthma control characteristics
and prevalence survey study (access). The Journal of Pediatrics, 157(2), 276-281.
Objective 4-Psychosocial Effects of Hospitalizaiton

According to Hockenberry and Wilson (2009), often illness and hospitalization are the first crises children will experience. Because of their striving for independence and productivity, school age children are particularly vulnerable to events that may lessen their feeling of control and power (Hockenberry et al. 2009). Per Hockenberry et al.(2009), for school age children, dependent activities such as enforced bed rest, use of a bedpan, inability to choose a menu, lack of privacy, help with a bed bath or transport by a wheelchair or stretcher can be a direct threat to their security. However, when children are allowed to exert a measure of control, regardless of how limited it may be, they generally respond well to any procedure (Hockenberry et al. 2009). Some of the most cooperative, satisfied, and contented patients are school age children who help make their beds, choose their schedule of activities and assis in their own care. An increase sense of control usually results from a feeling of usefulness and productivity (Hockenberry et al. 2009). According to Hockenberry et al., (2009), illness may also cause a feeling of loss of control and one of the most significant problems of children in this age group is boredom; when physical or enforced limitations curtail their usual ability to care for themselves or to engage in favorite activities, school age children generally respond with depression, hostility or frustration. Per Hockenberry et al., (2009), one of the factors influencing the amount of stress imposed by hospitalization is the amount of control that persons perceive themselves as having; lack of control increase the perception of threat and can affect children's coping skills; many hospital situations decrease the amount of control a child feels.
Hospitalization is a major stressful experience for children. The impact of an unanticipated, critical care hospitalization on children and their families can be profound according to Small, Melnyk and Sidora-Arcoleo (2009). Coping response to hospitalization have found that emotional and behavioral sequelae are common following this experience. According to Small et al., (2009), 64% of all children admitted to a hospital are less than 10 years of age. The most common reactions to hospitalization include (a) separation anxiety, (b) detachment, (c) regression, (d) sadness, (e) apathy or withdrawal, (f) hyperactivity and (g) aggression (Small et al., 2009). Additionally, childhood hospitalization may also result in (a) loss of newly acquired developmental skills, (b) developmental delays, (c) loneliness and (d) isolation. Childhood hospitalization research indicate that children appeared to be more sensitive to specific stressors, such as separation from parents, instrumentation, unfamiliar environments and furnishings, and forced and intense interaction with stranger (Small et al., 2009).
Per Crole and Smith (2012), nurses are required to make decisions that affect the trust that has developed between themselves and the child. Decisions include the degree of control given to the child during their treatment, how much information to share with the child concerning upcoming events and whether or not parents should participate. According to Crole et al., (2012), building-trusting relationships with children is achieved through a nurse's use of appropriate language, games and play, adequate preparation of a child for procedures, and providing explanations and encouragement. Per Crole et al., (2012) giving the child some control is a common method used once trust has been established. In general, there are no guidelines that regulate nurses' delegating care tasks to children and allowing them to participate. However, to the extent possible, nurses reinforce the child's use of coping strategies that lead to healthy outcomes by giving options whenever it is safe to do so.
According to Wright and Newman-Giger, (2010), nationally, children of Hispanic origin are one of the most rapidly growing population groups in the United States. National data indicate that nearly 24% of Hispanic children are uninsured, representing the largest number of uninsured children in the United States, Wright et al., (2010). Language problems can result in adverse health consequences for some children, including poor medical care, misdiagnosis, and inappropriate medication and hospitalization. Low family income is an important independent risk factor among Latino children for suboptimal health and high utilization of health services. According to Wright et al., (2010) recently there has been an influx of research in the area of child health and how one’s family and one’s social environment can influence this. However, few studies have looked at the specific child, family, socioeconomic, and social factors that affect African American and Hispanic children Wright et al., (2010).
As stated by Rew, Principe and Hannah (2012), high levels of stress among racial and ethnic minority adolescents have been associated with social disadvantage and lower perceived socioeconomic status. According to Rew et al., (2012), boys, more than girls, experienced an increase in the intensity and overall experience of stress, whereas girls, more than boys, used more coping strategies and found them more effective over time. Non-Hispanics and girls, unlike Hispanics and boys, reported statistically significantly more frequent use of several coping strategies over time such as “pray” or “try to relax, stay calm.” Although the effectiveness of coping strategies significantly decreased over time, they remained significantly more effective for girls and non-Hispanics than for boys. One noteworthy exception was the strategy, “hit, throw or break things,” which increased in both frequency and intensity over time for boys only. This result may reflect a gender role difference in externalizing behaviors such as aggression and destructiveness; others have reported that boys used more avoidant and aggressive coping strategies than girls, Rew et al., (2012).
Rew et al., (2012), also states that children learn new coping strategies as they mature. A coping strategy such as hugging a stuffed animal, which may have been effective in Grade 4, may be replaced with coping by talking with a trusted adult, for example, as a child gets older and we found that “watch TV or listen to music” and “draw, write or read something” were the top two coping strategies used by school-age children, Rew et al., (2012).
According to Bai, Hillemeier, and Lengerich (2007), Black and Hispanic children with asthma are known to be at increased risk for hospital admission and hospital admission in turn has been associated with severity of symptoms at presentation to the emergency department. In a study done regarding asthma and school age children during hospitalization, Horner, Brown and Walker (2012) report both Hispanic and African American children reported they were more bothered by their asthma in general and specifically more bothered by their asthma symptoms than the non-Hispanic White children. Hispanic children had significantly higher (worse) emotional functioning PAQOL (Pediatric Asthma Quality of Life) than did non-Hispanic White children. Neither coping frequency nor asthma severity was statistically significantly different between racial/ethnic groups. According to Horner et al., (2012), a unique finding in this study was the significantly worse emotional functioning reported by the Hispanic children in comparison to the non-Hispanic White and African American children. The emotional function PAQOL subscale items addressed how often children feel angry, worried, concerned, or troubled because of their asthma and how often they feel frightened by an asthma attack, Horner et al., (2012).
Varela, Sanchez-Sosa, Biggs and Luis (2008) states in terms of severity and content of anxiety and fears, the literature points to more similarities than differences between Hispanic and European American youth (e.g., in social anxiety). Ethnic differences that have been found between these two broad cultural groups, most point to a pattern of greater anxiety and fear expression by Hispanic youth in areas such as health or somatic symptoms, fears of the unknown and of danger and death, general and health related worries, and rates of separation anxiety disorder, Varela et al. (2008). Varela et al., (2008) also indicates Hispanic youth reported more general worry symptoms than the European American groups. Girls reported higher physiological anxiety, worry symptoms, separation anxiety symptoms, social anxiety symptoms, fears of the unknown, and fears of danger and death than boys independent of cultural group.
References:
Hockenberry, M. and Wilson, D. (2009). Wong's Essentials of Pediatric Nursing. St.
Louis, Missouri: Elsevier Mosby.
Small, L., Melnyk, B. and Sidora-Arcoleo, K. (2009). The effects of Gender on the coping
outcomes of young children following an unanticipated critical care hospitalization.
Journal for Specialists in Pediatric Nursing, 14(2), 112-122.
Crole, N. and Smith, L (2012). Examining the phases of nursing care of the hospitalized
child. Australian Nursing Journal, 30.
Wright, K. and Newman-Giger, J. (2010). California’s young Hispanic children with
Asthma: Disparities in health care access and utilization of health care services.
Hispanic Health Care International, 8(3), 154-164.
Varela, R., Sanchez-Sosa, J., Biggs, B., Luis, T. (2008). Anxiety symptoms and fears
in Hispanic and European American children: Cross-cultural measurement
equivalence. Journal of Psychopathology & Behavioral Assessment, 30, 132-145.
Horner, S., Brown, S., Walker, V. (2012). Is rural school-aged children’s quality of life
affected by their responses to asthma? Journal of Pediatric Nursing, 27, 491- 499.
Bai, Y., Hillemeier, M., and Lengerich, E. (2007). Racial/ethnic disparities in symptom
severity among children hospitalized with asthma. Journal of Health Care for the
Poor and Underserved 18(1), 54-61.
Rew, L., Principe, C. and Hannah, D. (2012). Changes in stress and coping during late
childhood and preadolescence. Journal of Child and Adolescent Psychiatric
Nursing, 25, 130-140.
Objective 5 - Gestational Diabetes

Diabetes first diagnosed in pregnancy is designated gestational diabetes Mellitus (GDM); most patients with GDM have features in common with type 2 diabetes, Childs, Cypress and Spollet (2005) p.3. According to Burrow, Duffy and Copel (2004) p. 35, GDM is defined as carbohydrate intolerance of varying severity with onset or first recognition during pregnancy, GDM encompasses three different conditions: (1) "true" gestational diabetes, which develops in the later half of the pregnancy as a result of the altered hormonal milieu; (2) previously unrecognized type 2 diabetes, which is discovered as a result of screening; and (3) the uncommon case in which the first manifestation of type 1 diabetes occurs when a woman is pregnant. GDM occurs more frequently in African American, Hispanic/Latino, and Native American populations. Approximately 4%of all pregnancies in the U.S. result in GDM, but the prevalence rate ranges from 1to 14% depending on the population studies. Although GDM is glucose intolerance during pregnancy, 5-10% of women with GDM are discovered to have type 2 diabetes, and women with a history of GDM have a 20-50% chance of developing diabetes over the next 5-10 years (Childs et al., 2005) p.5. Per Hedderson, Ehrlich, Sridhar, Darbinian, Moore and Ferrara, (2012), the prevalence of GDM has increased in all racial/ethnic groups, and this has been observed in several populations in recent decades.
According to Childs et al., (2005), women who are obese or have a prior history of GDM, a family history of diabetes, or glycosuria should have glucose screening done as soon as possible. Other women who are of average risk, older than age 25 years, overweight, or a members of a high –risk ethnic group or have a history of poor obstetrical outcomes (e.g., spontaneous abortion, congenital malformation, fetal macrosomia) should be screened for GDM at 24-28 weeks’ gestation. According to Werner et al., (2012), a common standard of current care, women universally received a 50-g 1 hour glucose challenge test (GCT) between 24-28 weeks. Women who failed the initial screening GCT received a diagnostic 3hour 100g-glucose tolerance test (GTT). Women with at least two elevated values based upon the Carpenter and Coustan diagnostic criteria were classified as having GDM, Werner et al., (2012). According to Lewis et al., (2011), the American Diabetes Association has made a new recommendation for women who are at high risk for gestational diabetes to be screened at the first prenatal visit using standard diagnostic testing. These pregnancies are at risk for a host of obstetric complications including preeclampsia, preterm labor, cesarean delivery, neonatal hyperbilirubinemia, shoulder dystocia, and birth injury. Recent studies have demonstrated that screening for and managing GDM mitigates many of these pregnancy complications and improved perinatal outcomes, Werner et al., (2012).
According to Hayes, (2012) pregnancy has long been termed a diabetogenic condition, primarily due to the physiological impact of placental hormones, which directly impact on the ability of insulin to function in maintaining euglycaemic control. According to Childs et al., (2005), "late pregnancy is characterized by accelerated growth of the feto-placental unit, increasing plasma concentrations of several diabetogenic hormones, including human placental lactogen and estrogens, and increasing insulin resistance. The parallel development of insulin resistance and increases in blood levels of human placental lactogen and other diabetogenic hormones, including cortisol, progesterone, and estrogens, suggest that these hormones are responsible for much of the observed insulin resistance. In healthy pregnant women, insulin secretion must be increased by 200-300% in late gestation to overcome the resistance and maintain euglycemia. The insulin resistance of pregnancy leads to hyperglycemia in susceptible women that often resolves after delivery but may recur in subsequent pregnancies" p. 9. Consistent with this pathogenesis, women who had GDM are at increased risk of developing diabetes later in life and should be screened for the subsequent development of diabetes through out their lives (Childs et al., 2005) p. 9.
According to Childs et al., (2005), "the main goal of management for pregnancies complicated by diabetes is to achieve and /or maintain euglycemia through out gestation. The treatment approach requires a combination of medical nutrition therapy, exercise, insulin therapy and daily multiple blood glucose determinations. The goals of nutrition therapy are to provide adequate maternal and fetal nutrition, to achieve appropriate gestational weight gain and to minimize glucose excursions. Mild exercise in the form of walking is possible for most women and has been reported to improve lipid profiles and blood glucose control. In regard to GDM, exercise has been recommended as an adjunct to nutritional therapy" p. 275. Per Childs et al. 2005, in the U.S., insulin is currently the only therapy recommended to treat diabetes during pregnancy. The goal of insulin therapy is to achieve blood glucose levels that are nearly identical to those observed in healthy pregnant women and human insulin is the least immunogenic of all insulin and is exclusively advised for use in pregnancy (Childs et al., 2005 p. 275). According to Dupak and Trujillo (2007), poor maternal glycemic control can result in maternal complications, such as high-degree perineal tears during delivery of a macrosomic infant and caesarean section resulting from failure of labor to progress. Fetal or neonatal complications can be significant and include sudden intrauterine death, shoulder dystocia resulting in brachial plexus injuries, intrauterine hypoxemia and neonatal hypoglycemia.
Nursing goals: Educate the GDM patient regarding dietary changes to promote adequate weight gain and maintain consistent blood glucose levels. According to Werner et al. (2012), GDM women received interventions including nutritional counseling and instruction and supplies for home glucose monitoring. On the basis of several studies, identifying and managing women with GDM improved perinatal outcomes (Werner et al., 2012).
It is important to teach the GDM patient about exercise and the need to monitor blood glucose before and after exercise. According to Childs et al., (2005) p. 275, regular aerobic exercise has been shown to lower fasting and postprandial glucose concentrations. Several randomized controlled trials have demonstrated that upper-extremity exercise for 20 min three times a week can significantly lower blood glucose levels in women with GDM. In addition, these trials found no significant increase in either maternal or neonatal complications.
References:
Hedderson, M., Ehrlich, S., Sridhar, S. Darbinian, J., Moore, S., Ferrara, A. (2012).
Racial/ethnic disparities in the prevalence of gestation diabetes mellitus by bmi.
Diabetes Care, 35,1492-1498.
Childs, B., Cypress, M., Spollett, G. (2005) Complete Nurse’s Guide to Diabetes Care.
Alexandria, Virginia: American Diabetes Association, pg. 1-2.
Werner, E., Pettker, C., Zuckerwise, L., Reel, M., Funai, E., Henderson, J. and Thung,
S. (2012). Screening for gestation diabetes mellitus: Are the criteria proposed by
the International Association of the Diabetes and Pregnancy Study Groups cost
effective? Diabetes Care, 35(3), 529-535.
Hayes, C. (2012). Gestational diabetes mellitus-why awareness is paramount. British
Journal of Healthcare Assistants, 6(1), 28-31.
Dupak, J. and Trujillo, A. (2007). Ultrasound surveillance in pregnancy complicated by
diabetes. Diabetes Spectrum, 20(2), 89-93.
Lewis, S., Dirksen, S., Heitkemper, M., Bucher, L. and Camera, I. (2011). Medical-
Surgical Nursing. Assessment and Management of Clinical Problems. St. Louis,
Missouri: Elsevier Mosby.
Objective 6 - Fetal Surveillance
Diabetes complicating pregnancy is a problem for which fetal surveillance testing is considered to be the standard of care according to Nageotte (2008). It is clear that control of diabetes throughout gestation, not just in the later stages, is more important for optimal outcome than is a specific form of fetal testing. Biweekly testing has become the standard and with well-controlled diabetics, allow gestation to continue until the onset of spontaneous labor, even when the gestation exceeds 40weeks, is appropriate management with normal testing (Nageotte 2008). According to Childs et al., (2005), all pregnancies complicated by diabetes require additional fetal evaluation and assessment. P. 276.
According to Dupak and Trujillo (2007), many studies have documented the relationship of maternal hyperglycemia on the degree of damage to women and their fetuses (i.e., maternal vessel disease, fetal malformation, obstetric and pediatric complications related to fetal macrosomia, and long-term health risks). The challenge of avoiding these complications lies in the unique ecology of the joint maternal-fetal metabolism and the maternal-fetal interchange circuit of the placenta (Dupak et al., 2007). Dupak et al., (2007) state that during pregnancy complicated by diabetes, the results of fetal surveillance testing will correlate with the degree of maternal glycemic control.
According to Dupak et al., (2007), ultrasonography is a noninvasive, readily available method to assess and monitor the fetus and is also a helpful guide for instituting early therapeutic management for pregnancies complicated by diabetes. Fetal ultrasonography in the first trimester or early in the second trimester allows confirmation of gestational age and helps to verify the absence of any malformations. A fetal echocardiogram in mid-pregnancy is used to screen for congenital heart defects. Serial ultrasounds thereafter are used to assess fetal growth, measure amniotic fluid volume, and evaluate the placenta, Childs et al., (2005) p. 276. Dupak et al., (2007) state the inaccuracy and poor prediction of fetal weight and the lack of practical alternative parameters, obstetricians still feel compelled to use ultrasound to guide obstetrical management of pregnancies complicated by diabetes, and especially to plan the time and mode of delivery to avoid a potential adverse outcome for pregnant women and infants.
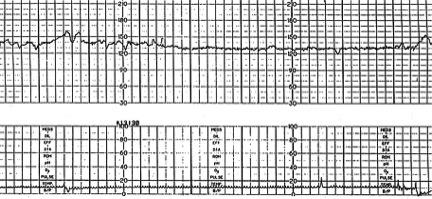
FIGURE 1.
Reassuring pattern. Baseline fetal heart rate is 130 to 140 beats per minute (bpm), preserved beat-to-beat and long-term variability. Accelerations last for 15 or more seconds above baseline and peak at 15 or more bpm. (Small square = 10 seconds; large square = one minute).
Tests for fetal assessment include non-stress fetal heart rate monitoring, contraction stress testing, sonographic biophysical profile including amniotic fluid measurement, Doppler studies and maternal assessment of fetal activity (Dupak et al., 2007).
According to The American Congress of Obstetricians and Gynecologists, "the nonstress test is the most common special fetal test. It measures the baby’s heart rate in response to the baby’s own movements. It is done to assess the health of the baby. For this test, two belts are placed across the abdomen: one belt has sensors that measure the fetal heart rate and the other belt has sensors to detect uterine contractions. The mother is asked to note when the baby moves by pressing a button, which indicates on the fetal heart rate record when a movement has occurred".
A biophysical profile may be done if a woman is past her due date or if she has a condition that causes fetal growth or amniotic fluid problems. It helps assess fetal well-being in these five areas:
1. Fetal heart rate
2. Fetal breathing movements
3. Fetal body movements
4. Fetal muscle tone
5. Amount of amniotic fluid. The modified BPP combines a nonstress test with an amniotic fluid assessment that is performed using ultrasound. The fetal heart rate is monitored in the same way it is done in the nonstress test. Ultrasound is used to measure the depth of the amniotic fluid in the uterus. If the amniotic fluid level is low, it could mean that there is a problem with blood flow in the placenta. According to Dupak et al., (2007), the amniotic fluid measurement has the best predictive value regarding perinatal morbidity; a measured amniotic fluid <2cm is considered to be significantly reduced and should prompt delivery.
The contraction stress test assesses how the fetal heart rate reacts when the uterus contracts. It sometimes is used if a nonstress test result is nonreassuring. In this test, belts with sensors that detect the fetal heart rate and uterine contractions are placed across the abdomen. To make the uterus contract mildly, the pregnant woman may be asked to rub the nipples through the clothing or she may be given oxytocin through a vein. The uterus may contract on its own, especially if the test is done late in pregnancy. A decrease in heart rate after most contractions is a nonreassuring result. For some women, this test may increase the risk of complications. The contractions could cause labor to start if the pregnant woman is at risk of preterm delivery. Also, the test may cause bleeding if patient has a condition called placenta previa or other conditions. ACOG.
References:
Nageotte, M. (2008). Antenatal testing: diabetes mellitus. Seminars in Perinatology, 32(4),
269-270.
Childs, B., Cypress, M., Spollett, G. (2005) Complete Nurse’s Guide to Diabetes Care.
Alexandria, Virginia: American Diabetes Association, pg. 1-2.
Dupak, J. and Trujillo, A. (2007). Ultrasound surveillance in pregnancy complicated by
diabetes. Diabetes Spectrum, 20(2), 89-93.
http://www.acog.org/Search?Keyword=non+stress+test. Accessed October 2012.
References:
Bai, Y., Hillemeier, M., and Lengerich, E. (2007). Racial/ethnic disparities in symptom
severity among children hospitalized with asthma. Journal of Health Care for
the Poor and Underserved 18(1), 54-61.
Black, J. (2011). What are patients’ priorities when facing the end of life? A critical
review. International Journal of Palliative Nursing, 17(6), 294-300.
Childs, B., Cypress, M., Spollett, G. (2005) Complete Nurse’s Guide to Diabetes Care. Alexandria,
Virginia: American Diabetes Association, pg. 1-2.
Crole, N. and Smith, L (2012). Examining the phases of nursing care of the hospitalized
child. Australian Nursing Journal, 30.
Dupak, J. and Trujillo, A. (2007). Ultrasound surveillance in pregnancy complicated by
diabetes. Diabetes Spectrum, 20(2), 89-93.
Hayes, C. (2012). Gestational diabetes mellitus-why awareness is paramount. British Journal of
Healthcare Assistants, 6(1), 28-31.
Hedderson, M., Ehrlich, S., Sridhar, S. Darbinian, J., Moore, S., Ferrara, A. (2012). Racial/ethnic
disparities in the prevalence of gestation diabetes mellitus by bmi. Diabetes Care, 35,
1492-1498.
Hockenberry, M. and Wilson, D. (2009). Wong's Essentials of Pediatric Nursing. St.
Louis, Missouri: Elsevier Mosby.
Horner, S., Brown, S., Walker, V. (2012). Is rural school-aged children’s quality of life
affected by their responses to asthma? Journal of Pediatric Nursing, 27,
491- 499.
Lewis, S., Dirksen, S., Heitkemper, M., Bucher, L. and Camera, I. (2011). Medical-
Surgical Nursing. Assessment and Management of Clinical Problems. St.
Louis, Missouri: Elsevier Mosby.
Liu, A., Gilsenan, A., Stanford, R., Lincourt, W., Ziemiecki, R., and Ortega, H. 2010. Status of asthma
control in pediatric primary care: Results from the pediatric asthma control
characteristics and prevalence survey study (access). The Journal of Pediatrics,
157(2), 276-281.
Nageotte, M. (2008). Antenatal testing: diabetes mellitus. Seminars in Perinatology,
32(4), 269-270.
Nicholas, J. and Hall, W. (2011). Screening and preventive services for older adults.
Mt. Sinai Journal Medicine, 78(4), 498-508.
Pijnenburg, M. and Leget, C. (2007). Who wants to live forever? Three arguments
against extending the human lifespan. Journal Medical Ethics, 33, 585-
587.
Rew, L., Principe, C. and Hannah, D. (2012). Changes in stress and coping during late
childhood and preadolescence. Journal of Child and Adolescent
Psychiatric Nursing, 25, 130-140.
Small, L., Melnyk, B. and Sidora-Arcoleo, K. (2009). The effects of Gender on the coping
outcomes of young children following an unanticipated critical care
hospitalization. Journal for Specialists in Pediatric Nursing, 14(2), 112-
122.
Vance, D., Graham, M., Fazeli, P., Heaton, K., and Moneyham, L. (2012). An overview
of nonpathological geroneuropsychology: Implications for nursing practice
and research. Journal of Neuroscience Nursing. 44, 43-54.
Varela, R., Sanchez-Sosa, J., Biggs, B., Luis, T. (2008). Anxiety symptoms and fears in
Hispanic and European American children: Cross-cultural measurement
equivalence. Journal of Psychopathology & Behavioral Assessment, 30,
132-145.
Werner,E., Pettker, C., Zuckerwise, L., Reel, M., Funai, E., Henderson, J. and Thung, S. (2012).
Screening for gestation diabetes mellitus: Are the criteria proposed by the
International Association of the Diabetes and Pregnancy Study Groups cost
effective? Diabetes Care, 35(3), 529-535.
Wright, K. and Newman-Giger, J. (2010). California’s young Hispanic children with
Asthma: Disparities in health care access and utilization of health care
services. Hispanic Health Care International, 8(3), 154-164.
Yang, B.H., Mu, P.F., Huang, C.M., Lou, H.L. and Wu, K.G. (2012). Relationship among asthma
knowledge, behavior management and social adaptation in school age children with
asthma in Taiwan. Nursing and Heath Sciences, 14, 165-172.
http://www.acog.org/Search?Keyword=non+stress+test. Accessed October 2012.